
Honestly, the moment most people realize something is wrong with their joints… it’s not during exercise.
It’s something smaller.
Getting out of a car.
Standing up from a couch.
Walking down stairs in the morning.
I’ve watched this play out with friends, relatives, older neighbors, even people in their late 30s who assumed joint pain was “temporary.”
At first it’s brushed off.
“Probably just stiffness.”
“Maybe I slept wrong.”
“Must be aging.”
Then months go by.
The stiffness keeps showing up.
The knee clicks more.
The fingers feel swollen in the morning.
Eventually someone Googles the question almost everyone asks at that point:
“What is osteoarthritis?”
And here’s the strange part I’ve noticed after seeing so many people go through it…
Most people already have osteoarthritis symptoms long before they understand what it actually is.
And the misunderstanding is where most of the frustration starts.
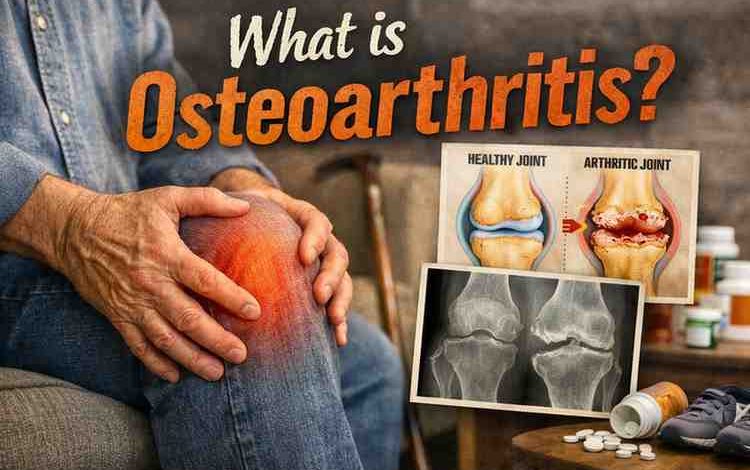
What Is Osteoarthritis (In Plain Human Terms)
From what I’ve seen, medical definitions often confuse people.
So here’s the simplest explanation that actually matches what people experience.
Osteoarthritis is gradual joint wear that happens when the protective cartilage inside a joint slowly breaks down.
Cartilage is basically the smooth cushion between bones.
When it’s healthy:
-
joints glide smoothly
-
movement feels quiet
-
pressure spreads evenly
When cartilage begins thinning or roughening:
-
bones rub more directly
-
inflammation appears
-
stiffness becomes common
-
pain appears during movement
Over time the joint becomes less efficient.
Not destroyed overnight.
Not suddenly broken.
Just… worn.
And that slow progression is exactly why people underestimate it.
Because the changes happen quietly for years.
The Pattern I’ve Seen Again and Again
Most people I’ve talked with about osteoarthritis share a weirdly similar timeline.
It usually unfolds in phases.
Phase 1 — Mild stiffness nobody worries about
This is where almost everyone ignores the signs.
Typical comments I hear:
-
“My knee just feels tight in the morning.”
-
“My hands take a minute to warm up.”
-
“My hip feels stiff when I stand.”
Pain level?
Usually very low.
Which is exactly why nothing changes yet.
Phase 2 — Movement starts triggering discomfort
Months later something shifts.
People begin noticing:
-
knee pain walking downstairs
-
hip pain after long sitting
-
finger stiffness gripping things
-
ankle discomfort after exercise
This is where people finally start researching what osteoarthritis is.
But here’s the surprising thing.
Most people at this stage still believe it’s temporary inflammation.
Not structural wear.
Phase 3 — The joint starts complaining daily
This is where frustration kicks in.
Symptoms become more consistent:
-
morning stiffness lasting longer
-
grinding or clicking sounds
-
swelling around joints
-
reduced range of motion
I’ve watched people reach this point and say: “I wish I paid attention earlier.”
And honestly… that’s extremely common.
Why People Develop Osteoarthritis
Most people assume osteoarthritis is simply aging.
But from what I’ve observed across different cases, it’s rarely just age alone.
Usually it’s a mix of things.
1. Joint overuse patterns
Athletes
Manual labor workers
Runners
Construction workers
Years of repetitive pressure can slowly wear cartilage.
Even fitness enthusiasts run into this if recovery is ignored.
2. Previous injuries
This one surprised me after hearing so many stories.
A knee injury in your 20s…
Can quietly turn into osteoarthritis in your 40s.
Old injuries change how joints distribute pressure.
Small imbalances build up over time.
3. Body weight pressure
Every extra pound increases load on weight-bearing joints.
Particularly:
-
knees
-
hips
-
lower spine
And most people don’t realize how dramatically this changes joint stress.
Even 10–15 pounds can shift joint mechanics.
4. Muscle weakness around joints
This is something physical therapists mention often.
Weak muscles mean joints absorb more force.
Strong muscles act like shock absorbers.
Without them, cartilage takes the hit.
5. Genetics
Some families simply develop osteoarthritis earlier.
Especially in:
-
hands
-
hips
-
knees
I’ve seen siblings experience similar joint issues within just a few years of each other.
What Osteoarthritis Actually Feels Like
People researching what is osteoarthritis often want to know something simpler:
“What does it actually feel like day to day?”
From what I’ve seen people describe, the feeling is very specific.
Common sensations
-
deep aching inside the joint
-
stiffness after inactivity
-
sharp pain during certain movements
-
grinding or popping sounds
-
reduced flexibility
Morning stiffness is incredibly common.
But interestingly…
It usually improves once people start moving.
That detail often surprises people.
The 5 Biggest Mistakes I See People Make
Almost everyone I’ve seen struggle with osteoarthritis makes at least one of these early on.
Sometimes several.
1. Waiting too long before addressing it
People assume pain must be “severe” before it deserves attention.
But early intervention helps the most.
The earlier people start adjusting movement and strengthening muscles…
The better the joint adapts.
2. Completely avoiding movement
This one is extremely common.
Pain shows up → people stop moving the joint.
Unfortunately, inactivity often makes stiffness worse.
Controlled movement is usually better than total rest.
3. Chasing miracle supplements
I’ve watched people spend hundreds of dollars on:
-
collagen powders
-
cartilage rebuild formulas
-
exotic joint pills
Some supplements may help symptoms slightly.
But they rarely reverse cartilage loss.
That expectation creates disappointment.
4. Ignoring muscle strengthening
Physical therapists almost always emphasize one thing:
Strong muscles protect joints.
Yet many people focus only on pain relief.
Not structural support.
5. Expecting quick fixes
Osteoarthritis changes happened slowly.
Recovery improvements also happen slowly.
Most people underestimate that timeline.
What Actually Helps (From What I’ve Seen Work)
Watching people manage osteoarthritis over time, certain strategies consistently help.
Not instantly.
But gradually.
Gentle strength training
Muscles around the joint absorb impact.
This often includes:
-
quadriceps strengthening for knees
-
glute strengthening for hips
-
grip exercises for hands
People who stay consistent here often report the biggest long-term improvements.
Low-impact movement
Activities that reduce joint shock:
-
swimming
-
cycling
-
walking
-
elliptical machines
These keep joints moving without excessive pressure.
Weight management
Even modest weight loss can reduce knee stress significantly.
Several people I’ve known noticed noticeable relief after losing 10–20 pounds.
Heat therapy
This surprised me.
Many people report heat helping more than ice for stiffness.
Warm showers or heating pads often ease morning stiffness.
Physical therapy guidance
People who work with trained therapists tend to learn:
-
proper movement mechanics
-
strengthening strategies
-
joint protection techniques
That guidance prevents many setbacks.
How Long Does Osteoarthritis Take to Progress?
One of the most common questions people ask.
The honest answer?
It varies widely.
Some people experience slow progression over decades.
Others notice faster changes after injuries or high-stress lifestyles.
From what I’ve seen:
-
mild symptoms can remain stable for years
-
lifestyle changes often slow progression
-
inactivity often accelerates stiffness
There’s no universal timeline.
But early management helps.
Reality Check Most People Need to Hear
This part can be frustrating.
But it’s honest.
Osteoarthritis currently cannot be fully reversed once cartilage is significantly damaged.
That said…
Symptoms can absolutely improve.
Pain can decrease.
Mobility can increase.
Daily life can become easier.
But it usually requires consistent habits.
Not one-time fixes.
Quick FAQ (Questions People Ask All the Time)
Is osteoarthritis the same as rheumatoid arthritis?
No.
Osteoarthritis is wear-and-tear joint damage.
Rheumatoid arthritis is an autoimmune disease attacking joints.
Completely different causes.
Can young people get osteoarthritis?
Yes.
Especially after injuries or intense joint overuse.
It’s less common but definitely possible.
Does cracking joints cause osteoarthritis?
No strong evidence supports that.
Joint cracking is usually gas bubbles releasing.
Is exercise safe with osteoarthritis?
Usually yes.
Low-impact strengthening often improves symptoms.
But high-impact activities may need adjustment.
Objections I Often Hear
“If cartilage is gone, what’s the point?”
This question comes up often.
Even if cartilage can’t fully regenerate, improving joint stability and muscle strength can still reduce pain dramatically.
Movement quality matters.
“Won’t exercise damage the joint more?”
When done correctly, exercise usually protects the joint.
The key is controlled strengthening, not high-impact strain.
“I’m too old to improve this.”
I’ve seen people in their 60s and 70s improve mobility significantly with gradual strength training and therapy.
Progress can happen at any age.
Who This Advice May Not Work For
It’s important to say this clearly.
These strategies may be limited for people with:
-
severe joint degeneration
-
advanced bone damage
-
complex inflammatory diseases
-
major structural deformities
In those cases, medical treatments or surgical options may be necessary.
And that’s okay.
Different stages require different approaches.
Practical Takeaways I Share With Friends
If someone asked me what actually matters most when dealing with osteoarthritis, I’d say this.
1. Pay attention early
Don’t ignore recurring stiffness.
Small signals matter.
2. Keep joints moving
Gentle movement prevents stiffness from locking in.
Stillness rarely helps long term.
3. Strengthen muscles around joints
Muscle support reduces joint stress dramatically.
4. Be patient with progress
Improvements often take months.
Not weeks.
5. Avoid miracle promises
Anything claiming to “rebuild cartilage fast” deserves skepticism.
And honestly…
What surprises people most about osteoarthritis is this:
It’s not always about eliminating the condition.
It’s about learning how to live well around it.
I’ve seen people go from frustrated and stuck… to managing their joints confidently once they understand how the condition actually behaves.
So no — it isn’t magic.
And yes, it can be discouraging at first.
But I’ve watched enough people regain comfortable movement after making small, consistent adjustments.
Sometimes that shift alone is the real relief.